

Few topics in anti-aging medicine generate more confusion — or more marketing spin — than bioidentical hormones. Patients arrive at consultations convinced that bioidentical hormones are “natural” and synthetic hormones are “chemicals,” that bioidenticals are unregulated by the FDA, or that switching from one to the other eliminates cancer risk. Most of that is wrong, and some of it is exactly backwards.
Here is the honest version. Bioidentical is a statement about molecular structure and nothing else. It means a hormone whose chemical structure is identical to what the human body produces — estradiol, progesterone, testosterone. It is not a claim about safety, source, or regulatory status. Many bioidentical hormones are FDA-approved prescription drugs sold by major pharmaceutical manufacturers. The distinction that actually matters clinically is not bioidentical versus synthetic. It is FDA-approved versus compounded. This guide walks through both comparisons, what the evidence supports, what it doesn’t, and how clinicians can counsel patients through a subject saturated with claims that outrun the data.
What “Bioidentical” Actually Means
A bioidentical hormone has the same molecular structure as the corresponding hormone produced endogenously in the human body. Estradiol prescribed as a patch is the same molecule as the estradiol produced by the ovary. Micronized progesterone is the same molecule as the progesterone produced by the corpus luteum. That structural identity is the entire definition.
Two things follow that patients rarely expect:
- Bioidentical does not mean the hormone came from a human, or from a plant, in any meaningful sense. Commercial bioidentical hormones are synthesized in a laboratory, typically starting from diosgenin, a plant sterol derived from soy or wild yam. Diosgenin is chemically and enzymatically converted through a multi-step process until the final molecule matches the human hormone. The starting material is botanical; the product is manufactured. The human body cannot convert diosgenin or yam extract into progesterone on its own — a persistent myth behind over-the-counter “natural progesterone” creams.
- Bioidentical hormones are drugs. They are prescription medications with pharmacology, dosing, contraindications, and adverse effects. The word carries no exemption from any of that.
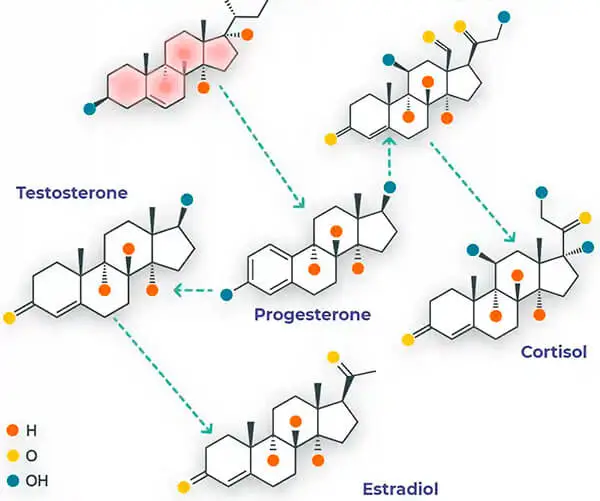
Bioidentical preparations exist across the endogenous steroid hormone families. The body produces more than a dozen endogenous steroid hormones, conventionally grouped into five classes:
- Estrogens — estradiol (E2), estrone (E1), estriol (E3)
- Progesterone
- Androgens — testosterone, DHEA, androstenedione
- Glucocorticoids — cortisol, cortisone
- Mineralocorticoids — aldosterone
All of these arise from a shared steroidogenic pathway, with enzymes converting precursors into downstream metabolites as physiologic demand shifts. That shared architecture is one reasonable argument for structural identity: a bioidentical molecule enters the pathway and is metabolized by the same enzymes, into the same metabolites, as the endogenous hormone. It is a mechanistically sensible rationale. It is not, by itself, outcome evidence — and the distinction between the two is where most bioidentical marketing quietly collapses.
What “Synthetic” Actually Means
“Synthetic” is a poor term, because bioidentical hormones are also synthesized. What people mean is non-bioidentical: a hormone-active molecule whose structure differs from anything the human body makes. It binds the same receptors, but not identically, and it does not necessarily produce the same downstream effects.
The two classic examples:
- Conjugated equine estrogens (Premarin®) — a mixture of estrogens derived from pregnant mare urine. It contains estrogenic compounds that do not occur in humans at all. CEEs were the dominant estrogen therapy for decades. Unopposed CEE use was subsequently associated with endometrial cancer in women with an intact uterus, which drove the practice of adding a progestogen.
- Medroxyprogesterone acetate (Provera®) and other progestins — synthetic compounds that act on progesterone receptors but are structurally distinct from progesterone. Adding a progestin addressed the endometrial cancer signal, but introduced its own trade-offs.
That last point deserves emphasis, because it is the single most consequential thing many prescribers get wrong: progestin is not progesterone. They are frequently treated as interchangeable in conversation and even in charting, and they are not the same drug. Progestins have distinct effects on lipid metabolism — generally raising LDL and lowering HDL relative to progesterone — and can markedly reduce sex hormone-binding globulin (SHBG). Lower SHBG means more free androgen available to bind receptors, which can produce androgenic effects patients did not sign up for.
Those trade-offs are a real part of why long-term adherence to conventional non-bioidentical regimens has historically been poor. A substantial share of women who start therapy discontinue it, often citing side effects or unresolved symptoms. Non-adherence is a clinical outcome in its own right, and it is not solved by telling patients the regimen works.
The Real Distinction: FDA-Approved vs. Compounded
This is the spine of the topic, and almost every article on it gets it wrong.
The common framing — “FDA-approved synthetic hormones versus unregulated bioidentical hormones” — is false. A large number of bioidentical hormones are FDA-approved, commercially manufactured, mass-produced prescription drugs, made under the same regulatory regime as any other pharmaceutical:
- Bioidentical estradiol — available FDA-approved as transdermal patches, topical gels, sprays, vaginal preparations, and oral tablets.
- Micronized progesterone — FDA-approved in oral capsule form since the 1990s. Micronization — reducing particle size to improve absorption — is what made oral bioidentical progesterone viable in the first place.
- Bioidentical testosterone — FDA-approved in multiple delivery forms.
So a clinician can prescribe bioidentical hormone therapy entirely within FDA-approved products, with known potency, verified batch consistency, standard labeling, an approved indication, and post-marketing adverse event surveillance. This is not a fringe approach; it is mainstream menopause care.
What is not FDA-approved is compounded bioidentical hormone therapy (cBHT) — custom preparations mixed by a compounding pharmacy, often as multi-hormone combinations at individualized doses, frequently guided by salivary or serial serum testing. Compounded preparations are made from the same bioidentical molecules, but the finished product has not been through FDA review. Notably, estriol has no FDA-approved product in the United States, so any estriol-containing regimen — including popular Bi-Est and Tri-Est formulations — is compounded by definition.
The practical differences between approved and compounded products are not abstract:
- Batch consistency. Compounding pharmacies are not held to the same manufacturing standards as pharmaceutical manufacturers. Potency can vary between batches and between pharmacies.
- Labeling. Compounded products do not carry the standardized labeling and warnings that accompany approved products — which means patients may receive an estrogen-containing product without the class warnings the FDA requires on its approved counterpart.
- Evidence base. Approved products reached market through clinical trials. Compounded formulations have not been studied to the same standard.
- Adverse event surveillance. Post-marketing safety monitoring for approved drugs has no real equivalent for custom compounded preparations.
Compounding has legitimate uses. A patient with a documented allergy to an excipient in every approved product, or who needs a dose or delivery route that no approved product provides, is a defensible candidate. “It’s more natural” is not a clinical indication. Major medical organizations have specifically cautioned against the marketing claims made for compounded bioidentical hormone therapy — not against hormone therapy itself, and not against bioidentical molecules, but against the assertion that compounded custom formulations are demonstrably safer or more effective than approved products. That distinction is worth defending in a consultation.
Delivery Methods: Where Bioidentical Therapy Genuinely Differs
The strongest practical argument for bioidentical hormone replacement therapy isn’t molecular mysticism — it’s that the available delivery options allow steadier levels and more granular dosing. Bioidentical hormones can be delivered by:
- Transdermal patches — deliver hormone at a controlled rate and bypass hepatic first-pass metabolism. This route difference is clinically meaningful and is one of the few areas where mechanism and evidence broadly agree.
- Topical creams, gels, and foams — also transdermal, though absorption depends on application site, skin condition, and adherence to technique. Transfer to partners and children is a real counseling point.
- Oral capsules — convenient; subject to first-pass metabolism. Oral micronized progesterone is often dosed at bedtime because of its sedating effect, which some patients experience as a benefit.
- Sublingual troches — rapid absorption, but levels can peak and trough sharply.
- Implantable pellets — inserted subcutaneously, typically in the upper gluteal area, releasing hormone gradually over several months.
Pellets deserve a straight assessment because they are heavily marketed. The appeal is real: sustained release, no daily adherence burden, no transfer risk, and stable levels compared with creams or troches. The trade-off is equally real: once a pellet is implanted, it cannot be dose-adjusted or removed easily if the patient over-responds or develops side effects. Insertion is a minor procedure with the usual procedural risks — site infection, bleeding, extrusion. And most pellet formulations used in the United States are compounded, placing them squarely in the category discussed above. Pellet therapy is a legitimate tool in trained hands, but it demands proper technique, careful patient selection, and honest consent — which is a reason to learn insertion through formal Hormone Pellet and BHRT Training rather than from a vendor rep.
What the Evidence Actually Says
Being candid here matters more than being persuasive.
What is reasonably well supported: Hormone therapy is effective for vasomotor symptoms and genitourinary symptoms of menopause. Route of administration affects risk profile. Micronized progesterone and progestins are pharmacologically distinct and should not be treated as interchangeable. Adding a progestogen protects the endometrium in women with an intact uterus receiving systemic estrogen.
Ready to put this into practice?
Explore Empire's hands-on, CME-accredited Functional & Regenerative Medicine courses — live patients, expert faculty, and ongoing mentorship.
What is plausible but not established: That bioidentical formulations, as a class, produce better clinical outcomes than non-bioidentical ones. The mechanistic rationale is sound and some comparative signals are encouraging — the progesterone-versus-progestin literature in particular has drawn considerable interest regarding differing breast tissue effects. But interest is not proof, and the comparative head-to-head research needed to settle it largely does not exist.
What is not supported at all: That bioidentical hormones are risk-free. That compounded bioidenticals are safer than FDA-approved bioidenticals. That “natural” hormones cannot cause the adverse effects associated with hormone therapy generally. That salivary hormone testing reliably guides dosing.
Patient-reported satisfaction with bioidentical regimens tends to be high. That is worth something — but satisfaction is confounded by individualized dosing, closer follow-up, longer visits, and the expectancy effects surrounding a treatment patients sought out and paid for themselves. Attributing all of it to molecular structure isn’t defensible.
Safety and Risks: The Unvarnished Version
No hormone therapy is risk-free, and bioidentical status does not confer immunity.
Estrogen therapy carries class-associated risks including thromboembolic events, stroke, and endometrial hyperplasia or carcinoma when unopposed in a woman with an intact uterus. These risks belong to estrogen as a pharmacologic class. Bioidentical estradiol is estrogen. Route and dose modulate risk; molecular structure does not abolish it.
Testosterone therapy carries its own considerations — erythrocytosis, acne, hair changes, effects on lipids and fertility, and in women, androgenic effects including voice change that may not be reversible.
Compounded preparations add a layer: potency variability, absent standardized warnings, and no trial data behind the specific formulation. When a patient on a compounded regimen has an adverse outcome, it is often impossible to know what dose they actually received.
Contraindications and cautions for hormone therapy generally include a history of estrogen-sensitive cancer, unexplained vaginal bleeding, active or prior thromboembolic disease, active liver disease, and known or suspected pregnancy. This is educational content, not individualized advice — candidacy is a decision for a patient and their own clinician.
Who Is a Candidate?
Hormone deficiency states in both men and women are associated with a meaningful symptom burden: fatigue, sleep disruption, mood changes, cognitive complaints, reduced bone density, and sexual dysfunction. Those symptoms are real, they are frequently dismissed, and untreated hormone deficiency carries costs of its own. The reflexive avoidance of hormone therapy following early risk headlines left a large number of patients undertreated — a genuine problem that the bioidentical marketing wave partly grew to fill.
Reasonable candidacy generally involves symptomatic patients with documented deficiency, evaluated with appropriate laboratory testing and clinical history, who understand what the therapy can and cannot do, and who have no contraindications. Age alone is not an indication. A patient with a bad lab value and no symptoms is not automatically a patient who needs treatment. Hormone therapy also isn’t a substitute for the fundamentals — patients frequently seek hormones for concerns that respond better to sleep, resistance training, and weight management. Practices treating this population often pair hormone services with physician-supervised medical weight loss, and the adjunct claims in that space deserve the same skepticism — see our look at whether MIC/B12 injections really work.
How to Counsel Patients on Bioidentical Hormones
Patients arrive pre-loaded with claims from podcasts, wellness influencers, and clinics with a financial stake in the answer. A few points make the conversation both honest and reassuring:
- Define the word. “Bioidentical means the molecule matches what your body makes. It doesn’t mean natural, and it doesn’t mean risk-free.”
- Correct the FDA myth immediately. Many patients are startled to learn that bioidentical estradiol and progesterone are FDA-approved. It reframes the whole discussion.
- Reframe the real choice. The decision isn’t bioidentical or synthetic — it’s approved product or compounded product, and what justifies going custom.
- Name the trade-offs of the delivery route the patient is asking for, especially pellets.
- Don’t oversell. Patients told a therapy is risk-free lose trust the moment they read anything else. Patients given the real picture tend to stay.
Frequently Asked Questions
Are bioidentical hormones safer than synthetic hormones?
Not established. There is a reasonable mechanistic argument and some encouraging comparative signals — particularly around micronized progesterone versus synthetic progestins — but the head-to-head outcome research needed to prove a safety advantage largely doesn’t exist. Route of administration and dose are better-supported risk modifiers than molecular structure. Anyone stating flatly that bioidenticals are safer is going beyond the evidence.
Are bioidentical hormones FDA approved?
Many are. FDA-approved bioidentical products include estradiol in patches, gels, sprays, and tablets; oral micronized progesterone; and testosterone in several delivery forms. What is not FDA-approved is compounded bioidentical hormone therapy — custom preparations mixed by a compounding pharmacy. Estriol has no FDA-approved product in the U.S., so any estriol-containing regimen is compounded. The widespread belief that “bioidentical” means “not FDA-approved” is simply false.
What is the difference between bioidentical and synthetic hormones?
Molecular structure. Bioidentical hormones are structurally identical to the hormones the body produces — estradiol, progesterone, testosterone. Non-bioidentical (“synthetic”) hormones are hormone-active molecules that differ structurally, such as conjugated equine estrogens derived from mare urine, or progestins like medroxyprogesterone acetate. Both categories are manufactured in laboratories. Both are drugs. The difference is what the molecule looks like, not whether it came from nature.
Are compounded bioidentical hormones covered by insurance?
Usually not. FDA-approved hormone products are commonly covered under standard prescription benefits. Compounded preparations and pellet insertion are frequently paid out of pocket, since compounded formulations lack FDA approval and are often dispensed outside standard pharmacy benefit structures. Coverage varies by plan, and patients should verify before committing to a regimen — the cost difference over years of therapy can be substantial.
What are the side effects of bioidentical hormones?
The same categories as hormone therapy generally. Estrogen: breast tenderness, bloating, headache, mood changes, breakthrough bleeding, and class risks including thromboembolic events and endometrial effects when unopposed. Progesterone: sedation, dizziness, mood changes. Testosterone: acne, hair changes, erythrocytosis, and androgenic effects in women. Pellets add procedural risks such as site infection, bleeding, and extrusion, plus the inability to easily reverse the dose. “Bioidentical” does not mean side-effect-free.
Do bioidentical hormones cause cancer?
The honest answer is that they have not been shown to be free of the cancer risks associated with hormone therapy as a class, and marketing that implies otherwise is not supported. Estrogen therapy is associated with endometrial cancer when given unopposed to a woman with an intact uterus — bioidentical estradiol included. Breast cancer risk with combined therapy remains an area of active study, with meaningful interest in whether micronized progesterone differs from synthetic progestins; that question is not settled. What can be said plainly: no one should choose a compounded bioidentical regimen believing it removes cancer risk.
Train in Hormone Replacement Therapy with Empire Medical Training
Hormone therapy is one of the fastest-growing areas of clinical practice, and one of the easiest to do badly. The gap isn’t pharmacology — it’s that most clinicians finished training with a solid grasp of steroidogenic pathways and almost no instruction in applying them to a symptomatic 52-year-old sitting across the desk. That gap is where the marketing rushed in.
Empire Medical Training has trained physicians, NPs, PAs, and RNs since 1998. Our Hormone Pellet and BHRT Training is CME-accredited and hands-on, covering patient selection, laboratory interpretation, dosing across delivery routes, the approved-versus-compounded decision, complication management, and live pellet insertion technique under expert supervision. The goal is straightforward: to let you offer hormone therapy competently and describe it to patients accurately — without repeating claims the evidence won’t carry.



